The Ultimate Guide to Best Diet Medications: Integrating Clinical Innovation with Quality Weight Loss (2026)
The Intracellular Mechanics of Satiety
Modern options like semaglutide and tirzepatide work by mimicking natural incretin hormones. When these medications bind to the GLP-1 Receptor on a cellular level, they spark an intracellular chain reaction. This triggers an increase in cyclic adenosine monophosphate (cAMP), which activates downstream master signaling path networks like mTOR and PI3K. The result is a dual benefit: the pancreas optimizes glucose-dependent insulin secretion via GLUT pathways, while the brain receives a prolonged signal of full satisfaction, muting food cravings for hours.
The Big 7: Comparing FDA-Approved Weight Management Options
Finding the right approach depends heavily on your unique metabolic profile, medical background, and lifestyle preferences. Here is how the top seven clinical options compare:
| Medication & Brand | Type & Frequency | Primary Efficacy & Benefits | Key Considerations |
|---|---|---|---|
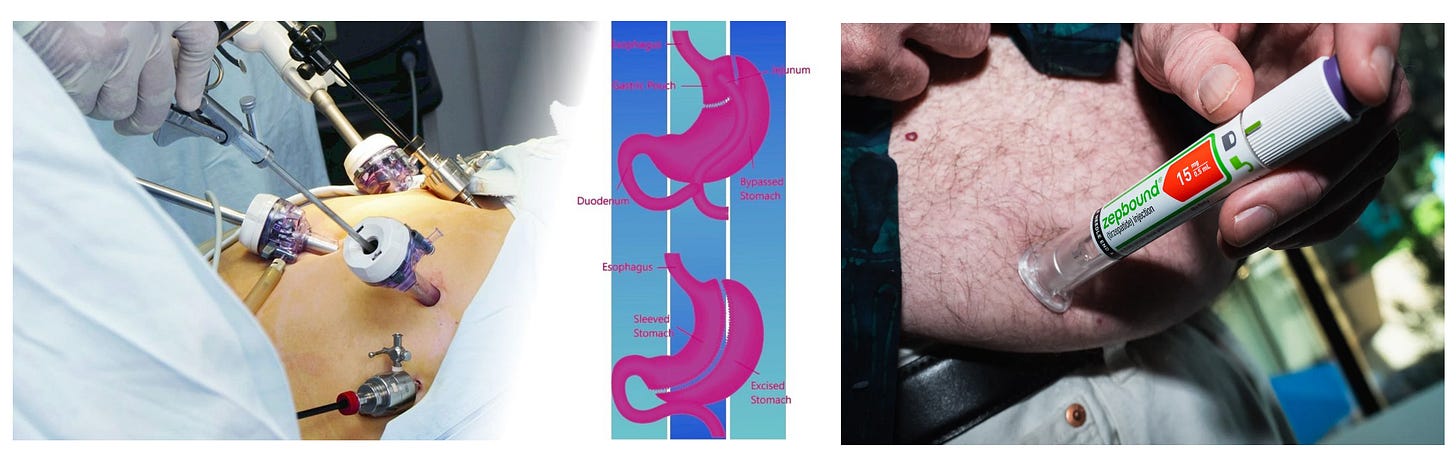
| Tirzepatide (Zepbound, Mounjaro) |
Weekly Injection | Highest average weight reduction (mean difference of negative 14.9% vs lifestyle alone). Dual GIP/GLP-1 agonist. | Requires strict titration; contraindicated in cases of personal or family history of Medullary Thyroid Carcinoma (MTC). |
| Semaglutide (Wegovy, Ozempic) |
Weekly Injection or Daily Pill | Average 15% weight reduction. Clinical data shows a 0.81 risk ratio reduction in all-cause mortality. | Oral tablet form must be taken on an empty stomach 30 minutes before any food or fluids. |
| Orforglipron (Foundayo) |
Daily Oral Pill | Non-peptide small molecule; highly stable absorption with no food or fluid timing restrictions. | Excellent option for individuals seeking an oral route without complex morning protocols. |
| Liraglutide (Saxenda) |
Daily Injection | First-generation GLP-1 receptor agonist; results in modest weight reduction (~5-8%). | Shorter half-life means it must be administered daily; often highly accessible via insurance plans. |
| Phentermine-Topiramate (Qsymia) |
Daily Oral Capsule | Combines a sympathomimetic stimulant with a neuro-anticonvulsant to dull appetite rapidly. | Requires baseline heart rate screening; strictly contraindicated during pregnancy. |
| Naltrexone-Bupropion (Contrave) |
Daily Oral Tablet | Targets neural pathways to suppress behavior-driven cravings, emotional eating, and habits. | Cannot be combined with chronic opioid use or history of uncontrolled blood pressure or seizures. |
| Orlistat (Xenical, Alli) |
Oral Capsule (With Meals) | Inhibits gastric and pancreatic lipases, blocking roughly 30% of dietary fat absorption in the gut. | Does not affect the brain. Can cause notable gastrointestinal changes if paired with high-fat meals. |
The Golden Rules for Body Composition & Muscle Preservation
When scale weight drops rapidly, your body can inadvertently pull energy from skeletal muscle mass. Clinical guidelines from the European Association for the Study of Obesity (EASO) highlight that the ideal objective is a 3:1 ratio of fat loss to lean-mass loss.
- Optimize Protein Architecture: Consume 1.2 to 1.5 grams of protein per kilogram of body weight daily to sustain muscle protein synthesis during periods of low caloric intake.
- Engage Mechanical Loading: Incorporate structured resistance exercises (weight training, bands, bodyweight movements) at least twice a week to cue muscle preservation pathways.
- Proactive Hydration: Incretin-based therapies frequently dampen natural thirst cues. Maintain a steady intake of 2 to 3 liters of water daily to protect baseline kidney and digestive function.
Navigating the Insurance Maze: A Step-by-Step Action Plan
Securing coverage for weight management medication requires deliberate document organization. Follow this roadmap to streamline the process with your medical provider:
- Document Baseline Biometrics: Ensure your medical chart explicitly lists your current Body Mass Index (BMI) alongside any weight-related comorbidities, such as hypertension, sleep apnea, or high cholesterol.
- Establish a History of Supervised Lifestyle Efforts: Many insurance plans require proof that you have participated in a structured diet or exercise plan for at least three to six months without achieving target health outcomes before approving advanced drug therapy.
- Request a Pre-Formulated Prior Authorization (PA): Have your physician use precise clinical language outlining that your medication is medically necessary for chronic metabolic disease management rather than cosmetic weight loss.
Disclaimer: This content is intended for educational purposes only and does not substitute for personalized medical diagnosis, advice, or treatment from a qualified healthcare professional.
Primary source:







Comments